Sportsmith Rehab Conference
I was lucky enough to attend the fantastic Sportsmith Rehab Conference earlier this month at the Etihad Stadium in Manchester. Below are some of the learnings and rough notes I took from the two days:
James Moore – Hip/Groin Pain
Kicking sports lead to pubic overload; straight line running leads to hip pathology
Hip joint a big player in groin pain – approx. 50% of cases have hip joint involvement. Arthrogenic muscle inhibition causes adductor overload. Hip micro-instability can do the same.
Anteverted hip joint will affect loading and how the muscles function.
Iliopsoas is an adductor as well as hip flexor, adductor magnus offloads hamstrings
In evasion team sports players cut stride length but this increases load through hip and hamstrings
Ratios important – hip flex/ext; abd/add
Stance leg function very important in kicking sports
Adductor muscle strength increases a lot U12-15 but tendon lags
Load abs in outer range, load them in extension
Short lever Copenhagen increased adductor load – eccentric between two plinths + 6kg weight is elite level
To increase adductor work in squat, depth is key rather than foot position
Use unilateral band work e.g. hip flex in SL bridge, hip add/abd in prone plank
Key references:
https://www.tandfonline.com/doi/abs/10.1080/14763141.2021.1951827 (Kicking biomechanics)
https://pmc.ncbi.nlm.nih.gov/articles/PMC4325295/ (kicking progression)
https://journals.healio.com/doi/abs/10.3928/01477447-20151228-08 (hip microinstability)
Seth O’Neill – Achilles Tendon
Tendon structure biggest risk factor for rupture – poor structure on screening 7x more likely to rupture – but doesn’t correspond to pain.
Can only rupture in pathological tendon – not necessarily painful prio
Soleus has largest physiological CSA – key propulser
When testing, have to compare to normative data rather than opposite limb
- Injured cohort weaker in both limbs
- Weaker muscle - greater tendon load
- IKD @90d/s >1.15x BW
Need to train with high loads - >90% MVC – and need to rehab in DF and “dirty” combined positions
Roula Kotsifaki – Jump Testing
Vertical hop 1/3 each from hip/knee/ankle
Horizontal hop only 13% contribution from knee – but is good for Ax landing strategy and forces
No need to measure hop distance as it adds nothing over the jump tests on force plate
6x BW landing force at end of triple hop
Cueing important:
- CMJ/SL “jump as high as possible”
- DL DJ/SL DJ “ jump as high and as fast as possible”
Squat jump best for Ax RFD
Main 4 variables:
- Jump height
- RSI
- Contact time
- Peak landing force – variance between R+L is normal
RSI often highlights biggest differences between limbs – linked to jump height
Force @ zero velocity also good to look at
With results look at LSI, pre-injury data, and normative data sets
Key reference:
https://bjsm.bmj.com/content/57/20/1304.abstract (jump testing)
Fearghal Kerin – Hamstring
Consider length, load and speed when selecting exercise
Banded ER (band around foot) a good way to increase BF activation during exercises
Introduce body contacts in hip hinge isometrics, etc
Is aponeurosis size a risk factor? Area of emerging research – as well as what exercise programme may change this
Villa research suggests T junction injuries more likely to break down in rehab
Romain Tourillon – Foot and Ankle
Foot and ankle important to “absorb, propel, recoil” – neuromuscular as well as structural
Important for robustness, performance, biomechanical efficiency

Need good intensity to train tib ant, post, peroneals – not just bands
e.g. shin bar, slant boards, iso catchs
Target strengthening into EOR DF ROM – strongest here and most functional
Involve mid-foot and 1st ray
Ankle DF during flight posture increase force output on jump testing

Testing KPI
SL HR>33
Tib post >35% BW
Tib ant 35-40% BW
Soleus >180% BW
Short presentations – Johan Lahti, Chris Bramah, Tom Dos Santos
Sprint technique changes with fatigue
Sprint technique can’t predict injury but can highlight those at risk
Anterior pelvic tilt/ trunk side flex alters trunk mm activity
This reduces horizontal force
Penultimate foot contact vital for COD
Key references:
https://www.mdpi.com/1660-4601/19/22/14643 (Fatigue)
https://journals.sagepub.com/doi/full/10.1177/03635465241235525 (S-MAS)
https://journals.sagepub.com/doi/abs/10.1177/1747954120922548 (Skill training)
Matt Taberner – Return to Performance
Performance means different things to different people. It is ill defined in the literature but research tends to agree a large proportion of players don’t return to pre-injury levels post long term injury.
Day 2
Brady Green – Calf Injuries
Identify risk factors at baseline and then address throughout the rehab
Indigenous athletes have increased risk and reduced SL HR performance
Hip function often poor – reduced proximal function can lead to calf overload
Calf strength should increase across season – if it’s not, may indicate issue
Soleus injuries on average 25 days to RTP – Grade 3 varies from 12-70 days – generally 4-8 weeks
Acute phase – approx. 4/7 to pain free walking
Palpation, ROM/tissue extensibility/ADLS/isolated PF key markers to exit this phase
Early rehab:
SL HR reps to failure aim for >25 @60bpm to transition out of this phase – cueing makes a big difference
Load isotonically in bent knee and straight knee positions
Test isometric capacity around 2/52 post injury
Progress walking drills to prep for running
Intermediate
As above plus directional power and SSC profiling
Aim for SL yielding isometric 1.5x BW
Pulsing exercises 100-160bpm
Higher bpm should have higher peak and average force – tidy up before high speed running
Testing RFD 1-3 reps 30/50/70/100% MVC
Straight knee PF in iso rig on force plates
Hinge with BB into step forward for horizontal force
PF in BB split squat for vertical force

SSC diagnostics:
Self-directed 20s hopping on force plate
Strict pogo
SL Squat Jump and SL CMJ – peak force >2000N
Prowler push for horizontal force development – 0.7-0.8xBW load -play around with trunk lean, A march, pushes
Keep monitoring once RTP – Ax data 6/52 prior to injury and then monitor for 16/52 post injury
“Don’t try to do everything, the exercise can be the test”
Alan Murdoch – Fit to Fast ACL Approach
Train high intensity movements as early as possible
Acceleration/upright max velocity/deceleration/change of direction
“Prep with purpose” – link to the above
Drill early to get fast
Less knee work with drill based running vs plod. More ankle work.
Tests for phase progression:
Return to function – hip ROM, trunk rotation
Return to run – quad strength
Return to sprinting – kinematic Ax
Return to COD/agility – reactive broad jump
Coaches Eye Ax:
Acc - “Throw to float” - Reduced power - Train with Leaning hip extension with band, ankle iso, heavy sleds
Max. V - “Studs to Jesus” - Reduced knee flex - Train with Knee flex, hip ext resisted step ups
COD - “Willow tree” - Lateral flex - COD isom, flamingos, banded lateral lunge
Decel - “Skimming stone” - Reduced ground contact - K box/overspeed decel/deep SLsquat
Simon Harries – Rehab Frameworks
Profile demands of the sport:
Attacking/defending
Tactical/technical
Physical load/actions
Consider linear, multi-directional speed agility (MDSA), and sport skills
Manipulate complexity, intensity, volume
Velocity drives intensity
MDSA manipulate: Changes in velocity, entry velocity, COD angle, time to prep
What to manipulate for on field rehab sessions:
% effort and space available
Task parameters
Sports skills

Drill type and movement opportunities – use constraints based learning design
Common approach makes it easier to individualise to the athlete in front of you.
Michael Giakoumis – Complex Hamstring
Ax - History, benchmarks, other considerations
Profile knee relative to hip
20-30% increase in hams work from 80-100% max. velocity
Negative work doubles
From 95-100% max. velocity load goes to ST>SM>BF
KPIs
Calf isom: 3.3-3.5xBW
Knee isom: 3.8-4.0xBW
Knee extension IKD >3xBW
Ankle PF seated isom 2xBW
Hip ratios – hip ext + abd = hip flex + add
Endurance
SL hams bridge 90/90 >30; NIRS rate of re-oxygenation
Force
90/90, 50/40, IKD
RFD
90/90 F@100ms
Tensile
Peak torque angle, outer ROM isom.
Co-ordination
2D/3D; Clinical Ax
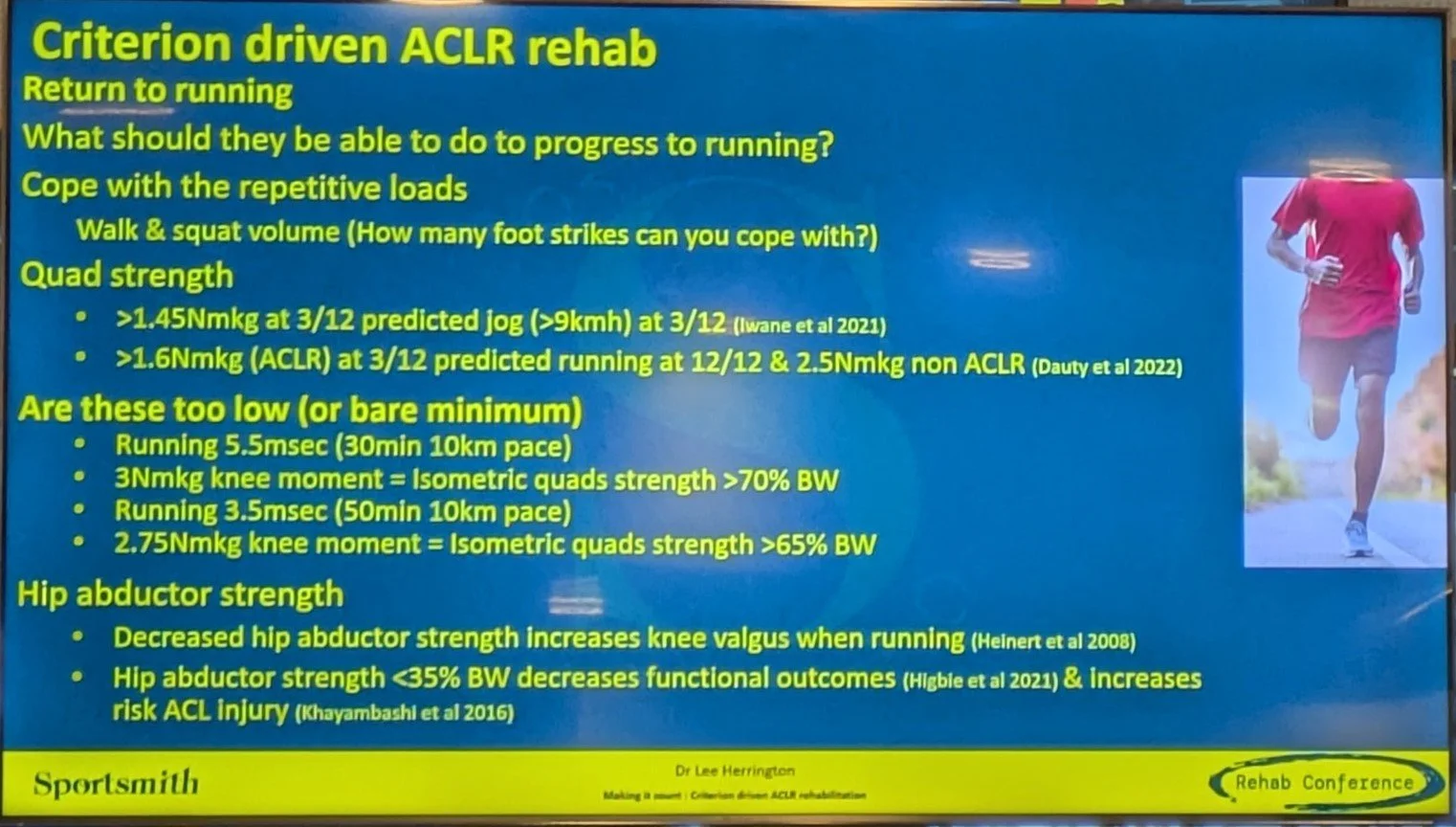
Lee Herrington – ACL
Start with the end in mind and then measure performance backwards
Initial markers:
Knee circumference a sensitive measure and will change across the day if knee not quiet
Step count a usual measure to quantify ADLs
Quads activation – SLR no lag the best we have clinically
Need full extension and functional flexion
DL squat to thighs parallel – use force plates to look at force distribution
Then:
SEBT – anterior reach 67% of leg length
1.5x BW – SL leg press or smith machine + 50% BW SLSq or step down
Isometric knee extension 3Nm/Kg
Hip abd >35% BW
LSI not useful – need benchmarks
Introduce vertical landings before horizontal – start with 2 up/1 down
For RT run:
Eccentric quad strength/step count/horizontal landing
Time on feet progression
Biomechanics related to greater quad and hams strength
For MD running:
Hop test performance key – use force plates not hop distance
Train penultimate foot contact
Ensure athlete can cope with addition of cognitive load
Use CMAS https://www.sciencedirect.com/science/article/abs/pii/S1466853X19301129
Build training volume in end stage
Treat like pre-season

FMPA Editorial
It was a real honour to be invited to contribute to the latest FMPA Magazine by Drs Andrew Shafik and Sean Carmody. Expanding on my previous blog posts on the rehabilitation of pars interarticularis injuries, I described some the aims as we progress the player during on-field rehabilitation.
If anyone wants to delve deeper into how we rehab these injuries in football then please don’t hesitate to get in touch.
Here’s the link for the magazine (subscription required)

Adolescent back pain - a pars injury rehab framework (Part 2)
In Part 1 I explained my framework for gym based progressions in the management of pars articularis injuries. In this second blog I will map out the basis of running and field based progressions to help take the player/patient/athlete from the gym floor all the way back to training. As I said in my previous blog, I am not saying this is the only way to approach the rehab of these athletes but hopefully people find it useful.
Reduced Weight Bearing
Reduced weight bearing running and sport/functional drills play a key part in getting the player comfortable and confident with sport specific movements.
If you are lucky enough to have access to a Hydroworx system, Alter G or similar (see below) then you can start running with a significant percentage of bodyweight offloaded.
A walk / run programme can commence with the run component initially being relatively slow and the overall volume of the session low. Over time you can manipulate the key variables – weight bearing, speed and volume. I see it almost like an equalizer where you may have to reduce one variable when progressing another, and looking to avoid progressing them all in one go.

If you have access to a pool with a varied or adjustable depth, multi-directional work can take place to help the player’s body start to adapt to the specific demands these movements place in a reduced weight bearing environment. This can involve reactive work in the latter stages as well as throwing and catching a ball even if the player usually uses their feet!
The pool can only really be progressed to about 60% weight bearing so an Alter-G treadmill can be used to bridge the gap between this and full weight bearing. The weight bearing percentage can be easily increased over a timescale agreed with the medical staff and external specialists. It is worth noting that there is research to suggest that increasing the running speed has a bigger impact on joint loading (albeit plantar force) than increasing weight bearing. This takes us back to my earlier point about being mindful not to increase weight bearing, speed, and volume all at the same time.
Outdoor Rehab
Once the player has progressed to 95%+ weight bearing then they can transition to pitch based work. In my experience players – and their backs - actually prefer the multi-directional nature of pitch based sessions to the extension biased treadmill running. At this stage weight bearing on our equalizer of parameters is replaced with intensity.
When planning, I work backwards from the provisional RTT timescale that has been proposed by the specialist. In my experience, a time frame of 6 weeks is advised to progress through reduced weight bearing modalities, onto the grass and then into modified training. This can be quicker if the injury has been a stress response rather than fracture, or longer if there are any potential complicating factors.
The first goal is to gradually build volume and this usually starts with a schedule of one day on grass followed by an indoor recovery day for an initial period. If this is comfortable, then the player may work outdoors on consecutive days but this somewhat depends on their normal training schedule and your access to the player.
Once the player can tolerate a sufficient amount of volume – active duration and GPS markers such as total distance and distance per minute can be useful to guide this – then we progress to add blocks of higher intensity work. This is initially in the form of more controlled work before progressing to more reactive work and position specific drills towards the end stage of outdoor rehabilitation. Matt Taberner’s work does a great job at outlining a framework for this. GPS measures can be useful to inform whether the player is at a level to drop into modified training but if you don’t have this technology than a simple rating of perceived exertion (RPE) from the player can give you good information about how hard they are working in specific drills and sessions.
Returning To Training
It is tempting to think for both you and the player that your job is done once they have returned to training. However they are likely to need their training load and content modified while they transition back into full training. There are no recipes for this and how this transition is managed will depend on the player, their position, the training schedule, the coaching staff, you and your team’s experiences, and a number of other factors.
I hope you’ve found these blogs a useful summary of my approach to rehabilitating these often tricky injuries. If you have any questions or comments, please don’t hesitate to reach out via email or social media.
Adolescent back pain - a pars injury rehab framework (Part 1)
If you work with adolescents, particularly athletic youngsters, you should know about Pars interarticularis injuries. This should be high up on the list of possible diagnoses whenever you see an active teenager with low back pain.
There are plenty of resources online (here for example) that outline the pathology in more detail but this blog is going to focus on the rehabilitation of these injuries. I will detail exercise selection and outline a framework for rehabilitation progression. I will follow this post up with a piece more focused on football specific, pitch based rehab progression.
Firstly, a disclaimer. If you are suspecting the patient/athlete in front of you has this type of injury, a specialist opinion from an orthopaedic or sports medicine colleague can be useful. They can organize the appropriate imaging to confirm the severity of the injury and determine the necessary offload from sport and activity.
As well as the above, it goes without saying that the process detailed below is the way I approach these injuries. I am not saying this is the only way to approach the rehab of these athletes but hopefully people find it useful.

With the gym based component of rehabilitation of this injury, I like to think of it as layering components of muscular function on top of one another (see above). Each component, once developed, works in synchrony with the others. Particular exercises will be able to be used to work on more than element whilst certain aspects may require very specific exercises or movements.
Although these exercises will be performed in the gym, I think its really important to keep the end of goal of what sports and activities the athlete will be returning to in mind. Its also important to identify the key movement patterns that need re-training. A diverse programme is likely to cover most bases but it is important to be specific to the athletes needs. For example, most athletes with this issue will benefit from controlling movement in all planes. But there is likely to be one or more directions that needs particular focus and you should weight your exercise selection and programming accordingly.
Assessment
I don’t think there is a particular assessment or test that will give you all the answers but taking a good history and establishing what the main aggravating or provocative movements have been will give you a good start. From there, and once you’ve carried out your physical assessment, observing and/or videoing the athlete perform a range of movement patterns can highlight what aspects need particular work to improve.
Control phase
For me, this is where the foundation for a successful rehabilitation is built. Depending on the outcome of your assessment it is likely to involve working on spinal dissociation and the ability to resist extension, rotation, and/or side flexion. Initially this ability might be focused on static positions but I always find it useful to assess this capability in dynamic positions early on. Whilst Pilates based exercises and other mat based variations can be useful, I like to include standing work from day 1. This might be in the form of pallof press variations (see below) or supported leaning tower or running man variations.
Strength & Endurance
It is often not necessary to change exercises in order to develop strength and endurance. I tend to focus on endurance earlier in the rehab process as I want the people I am working with to be able to maintain control (for want of a better term) during sporting activities that may last close to two hours. Because of this, fatigue resistance is an important quality to develop.
Strength is important to develop to ensure that the high forces involved in sporting activity are able to be resisted. Progressive overload in the movement patterns you are honing in on will help the athlete be able to do that. Ensure that the different positions that the athlete will find themselves in their sport are being addressed. Multi-directional lunge variations, step ups, are deadlifts are just a few to consider but don’t forget running specific postures.
Rate of Force Development (RFD)
An often neglected, but extremely important, component of gym based rehabilitation is to program exercises that develop power. A high rate of force development (RFD) is important in athletic tasks and the patient needs to be exposed to this in a progressive manner during their rehab to ensure that their body is used to working at high velocities. Examples include slams, throws, and catches in different positions.
Thanks for reading and I hope you find this of some use the next time you see an athlete with low back pain. I plan to post part two focussing on pitch based rehab in the next week or two. If you have any questions, please feel free to get in touch.
Physiotherapy in Wimbledon

Just a quick update to say that my clinical practice has moved location to Wimbledon.
I am now practising out of Mint Wellbeing which is based in Fitness Space Gym in central Wimbledon. The gym is kitted out with fantastic Technogym equipment which we are thankfully allowed to use for rehabilitation purposes whilst gyms are closed during lockdown.
The clinic is less than a minute from Wimbledon station and has ample parking nearby at Centre Court shopping centre providing great access from South West London and Surrey. It is also located just a 5 minute walk from the new Fortius Clinic site meaning that MRI scanning and expert Consultant opinions are literally just around the corner. I also see a great many patients referred from the excellent Consultants at nearby Parkside Hospital.
Despite the current lockdown we are open to see patients and have stringent PPE and cleaning procedures in place. Please contact me if you are interested in booking an appointment.
Growing Pains in Teenagers

With my experience working with young athletes at Chelsea’s Academy and England Hockey’s youth set up, I’ve developed an interest in the injuries that are unique to this age group. A quick Google search for information about “growing pains” often leads to information - including this page from the NHS - regarding this phenomenon in children under the age of 12. What about those aches and pains as teenagers go through their growth spurt?
What are some of the common growth related injuries?
Although they can occur in the upper limb, the most frequently seen conditions tend to be lower limb related.
Osgood - Schlatter’s
This is when pain is felt at the insertion of the quadriceps at the tibial tuberosity - basically the knobbly bit below the knee cap! Common in sports that involve running and/or football a lot of youngsters will experience pain in this area at some point around their growth spur.
Sever’s
This is the term given to pain at the back of the heel where the Achilles tendon connects onto the bone. As with Osgood-Schlatter’s this is common in running based sports but often starts at a younger age.
Pelvic Injuries
The two most common areas in this region to injure are the Anterior Inferior Iliac Spine (AIIS) at the front of the pelvis and the ischial tuberosity deep in the buttock. The AIIS is where the part of the quadriceps muscle - rectus femoris - originates and is susceptible to repeated and powerful kicking. The ischial tuberosity is where the hamstring originates so sprinting is the most common mechanism of injury.

Why might injuries occur?
The adolescent growth spurt is actually the second most rapid period of growth after the first two years of life. As teenagers go through this period, technically termed peak height velocity, they can grow over 10cm in a year. As well as this upward growth, they are likely to gain body mass as well lose some flexibility and co-ordination. Couple this with the other hormonal and developmental changes they are going through and it is clear to see why this can be a challenging period for many young athletes. There is some published research that suggests the risk of injury is higher during this period of change and we know there are some specific injuries that are only seen in these age groups.
It sounds obvious but one of the main reasons that adolescents have a specific injury profile is that their skeleton is still developing. Certain areas - such as the pelvis and spine - can even continue to mature into the early 20s!
Two areas in particular are at heightened risk of injury. The growth plate itself and the apophysis. This a bony tuberance where a tendon connects onto the bone. These areas are vulnerable to traction forces and are the areas affected in conditions such as Sever’s and Osgood-Schlatter’s Disease. These are the most commonly affected areas in young athletes although in sprinting and kicking based sports the attachments around the pelvis can also be vulnerable to injury.
In extreme cases can be pulled off the bone. This injury is called an avulsion fracture and whilst limiting initially it only warrants surgical intervention in extreme cases.
What can we do?
Every teenager is different but these strategies are the common ways to manage these types of injury:
Reviewing their weekly sporting schedule and ensuring they have an appropriate level of recovery time for their age group as well as variety across the week. If they are participating in one sport for more hours than their age (e.g. More than 14 hrs a week of football for a 14 year old) this might be a problem.
Carry out a thorough biomechanical assessment looking at joint range of movement, muscle flexibility, strength and co-ordination.
Use the assessment finding to put together a tailored rehabilitation program. Everyone is different so whilst some teenagers need to improve their strength, others might need to work on their flexibility or co-ordination, or both. There may well also be a role for manual therapy and/or taping depending on the presentation.
If symptoms have come on suddenly then diagnostic investigations such as an MRI, and an assessment with a sports physician might be warranted.
It is reassuring to know that most growth related issues improve relatively quickly, particularly if they are non-acute, with the right management plan.
If you have any specific questions, send me an email here
Physiotherapy after Orthopaedic Surgery
With elective surgery starting up again at places like Fortius Clinic and Schoen Clinic after the Covid-19 pandemic, I thought it would be useful to outline what to expect from physiotherapy during your post operative recovery. Whilst there will be some differences depending on the joint you have had operated on and the specific procedure that has been performed, the stages I have outlined below are applicable to most. Of course, always follow the advice of your surgeon and physiotherapist as this does not replace professional advice!

Immediate post-op phase
The focus initially is on reducing any swelling and being able to look after yourself at home. Don’t be scared to take your prescribed pain relief to help with this process and follow the instructions of your surgeon with regards to how much you are allowed to do. If you have had surgery on your lower half you may be on crutches and moving around with these can take a bit of practice. If you have had shoulder or elbow surgery you may be in a sling or brace which may restrict your ability to wash yourself and do the household chores.
In almost all cases you will have some ‘homework’ from your physio. This will normally comprise of gentle movement exercises and some gentle muscle activation work. Although these might be the last thing you want to do in this stage, they are really helpful in laying the foundations for the stages to come.
Regaining range of movement and muscle function
Some procedures mean that you are only allowed to move the operated joint a certain amount. This will be detailed in the post-operative instructions. But a lot has changed in recent years and now most of the time we are actively encouraged to move as much as possible. Aside from the obvious, movement is great at helping to reduce swelling and inflammation, and normalising muscle function. Pain and swelling have an inhibitory effect on muscles meaning that it can be hard to activate and get them going again after surgery. The longer this goes on, the longer the process to regain their strength and function.
Regaining everyday function
As range of movement and muscle function improves, you should find it much easier to do the things you need to across the day. This might mean getting rid of your crutches if you have had lower limb surgery, or being able to dress yourself easily if you’ve had shoulder surgery. As well as being great for your operated joint, it obviously makes life a whole lot easier.
Building strength and co-ordination
As pain decreases and function improves it is time to hit the gym! Don’t worry if you have not been to a gym much before, your physiotherapist should help guide you through the process of progressively loading the operated joint in a safe but challenging way. We have to challenge the muscles in order to regain strength so there will be some hard work involved but this will be really rewarding as you see your muscle bulk returning and gain confidence from feeling stronger. Co-ordination should improve as you become more practised at the exercises and over time the complexity of these will likely be progressed as well as the load you are working against. This is the stage where your physiotherapist can liaise with your personal trainer (if you have one) or may recommend the services of a strength and conditioning coach alongside physiotherapy sessions.
Return to sport
Obviously not everyone will be aiming to get back to sport on a regular basis but it is important when setting your goals with your physiotherapist to consider some of the things you do occasionally so that you can progress your rehabilitation program to an appropriate level to be able to complete these activities confidently and safely. Even if you only have the occasional kick around you will need to be able to change direction quickly, kick a ball and have the endurance to run for 30 mins plus. If you enjoy playing tennis on your summer holidays, we need to make sure that you are able to a swing a racquet, reach for those trickier shots and perfect those overhead smashes again.
Keep it Up!
This last stage does not necessarily need to involve a physiotherapist but it certainly can do. In order to maintain the improvements made during your rehabilitation and to minimise the risk of re-injury it is important to keep things ticking over. This doesn’t mean you have to be doing your physio exercises all day everyday, but it will involve keeping fit and active with some general exercise most days and continuing with some resistance training a couple of times a week.
If you are waiting for your surgery I hope this gives you a bit of insight into what to expect in your recovery but please get in touch if you have any specific questions or concerns about your rehabilitation.
Returning to Sports post Lockdown
Having been back in clinic at Complete Physio this week, as well as continuing online consultations, I have noticed a few common themes cropping up. In this post I will highlight some of the issues I have seen and how to reduce the risk of this happening to you.
Doing too much too soon
Whilst plenty of people have managed to stay active through the lockdown period with regular running, cycling and HIIT classes, one ‘trap’ I have noticed patients falling into is adding in lots of extra sessions in a short space of time especially in the nice weather. Whilst some will be able to cope with this for others this can lead to pain or injury.
Only having done body weight exercises for the last 3 months
Whilst this is better than nothing, it is really important to try and exercise using some additional resistance before returning to sports or significantly increasing your exercise volume. Our muscles adapt both ways to loading. we use this to our advantage whilst training and during rehab to get stronger using progressive overload but to put it bluntly if you don’t use it you lose it! Whilst this is frustrating, it is important to acknowledge this, and look to create your own progressive overload at home - particularly whilst the gyms are closed.
This point is also important to remember when gyms do re-open. It is unrealistic to think that you will be able to jump straight back in and use the same weights as three months ago.
Moving less
Even with exercising on a daily basis, you are still probably doing less than you would do commuting to the office, walking out for lunch, moving meeting to meeting. Just take a look at the step counter on your phone or Fitbit and compare the numbers to earlier this year. As well as this incidental exercise, the new way of working means that the meeting come to you. It is very easy therefore to jump meeting to meeting and not move from your chair all morning. Patients with back and neck pain find this particularly problematic but it is important for our whole body - and brain - to move!
Solutions
Here are three simple solutions to help you stay injury free.
Sometimes less is more
Although the 10% rule is not set in stone it can give you a good guide to help increase your activity levels while mitigating the risk of injury. If you need more detailed guidance or you have tried this already and are still having issues get in touch.
Get creative
You can use a range of different things to make up for not having weights. Bottles of water, a backpack full of books, all that pasta you panic bought, small children! Obviously use your common sense and only use what is safe for that exercise but the list is almost endless.
Move more
It sounds obvious but its as simple as that. Get up and do a lap of your makeshift desk between every meeting. Set a hourly reminder on Outlook. Little and often is key with this kind of thing.
I hope you find this post useful and don’t hesitate to drop me a line if you have any questions or want to discuss your injury to safe return to sport and exercise.
Back In Clinic!
My first (of many hopefully) blog post is to let everyone know that I will be back in clinic very soon.
From Tuesday 16th June, I will be back at Complete Physio Bury Street in the City one session a week. I will be available between 8am - 4pm on a Tuesday but appointments can be organised outside these times on request. Obviously things will be a little different with social distancing in the waiting room and PPE for both you and I but it is great to be able to offer this service again.
I will also be continuing to offer online and telephone consultations for the foreseeable future whilst people continue to work from home. As well as this, I have started to supervise outdoor rehabilitation sessions in local parks focusing on bodyweight exercises, running drills and sport specific rehab sessions. Just drop me an email (edclarkephysio@gmail.com) if you want to find out more.
Hopefully see you soon!